
Hip Pain associated with Impingement and Labral Tears

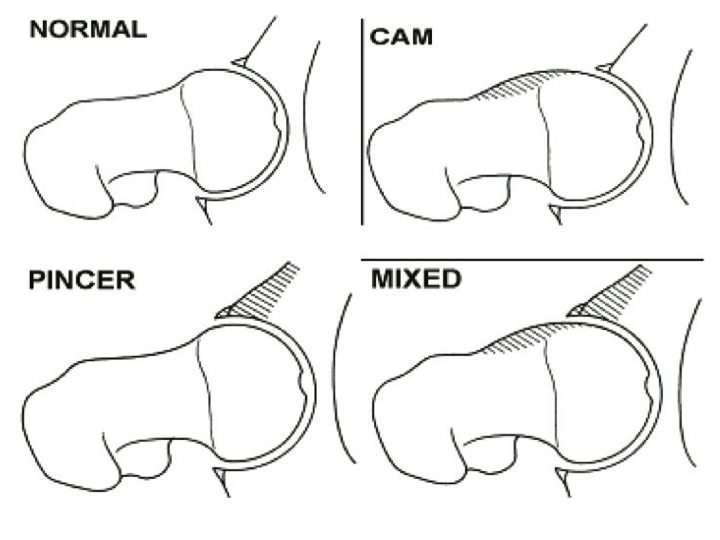
Femoral Acetabular Impingement (FAI) is defined as the mechanical abutment of the femoral head against the acetabulum1. This contact is either structural (cam or pincer lesion), functional or a combination of both and results in pain, loss of motion, and disability.
Researchers have questioned if the findings noted on x-ray are a normal morphological changes based on anatomy and biomechanics or a structural pathology(3).
These structural changes are apparent in asymptom- atic individuals and there are currently no randomized controlled trials showing they lead to early OA or hip surgery(2).
In a study of over 2000 asymptomatic hips authors noted labral and FAI bone changes in 68% and 67%, respectively. The prevalence of pathology consistent with FAI was higher in asymptomatic athletes(5). Pathology in asymptomatic hips also appears to increase with age(6).
Authors note an 18 fold increase in surgeries from 1999 to 2009 and a 365% increase in surgery between 2004 and 2009 among 20-39 year olds alone(4). This rapid increase in surgery is thought to be due in part to an increase in MRI being performed in this population.
Physical Therapy Solutions for Hip Pain
Conservative treatments are the first line of treatment for patients with anterior hip and groin pain resulting from labral tears or FAI. Interventions include activity modification, education, manual therapy (joint mobilization/ manipulation, soft tissue mobilization, and dry needling), self hip mobilizations, and exercise (stretching, strengthening, balance, and motor control) interventions.
Experts suggest a 8-12 week course of conservative care may improve decision making for possible surgical referral(3).
Ayeri et al. demonstrated a negative response to an injection predicts a negative outcome following surgery more than a positive response for a positive outcome after surgery(8).
Physical Therapy Evidence for Treating Hip Pain and Injuries
Evidence for the conservative treatment of FAI lesions is currently at a case series level of research for both conservative and surgical treatments. To date no randomized controlled trials or long term data exist on surgical outcomes.
Kemp et al. documented poor outcomes for patients undergoing FAI surgery with greater chondral damage and those over age 40(9).
Hunt et al. found a multimodal treatment approach consisting of manual therapy, exercise, and education reduced lower quar- ter impairments and improved function at both short and long term outcomes(7).
In our experience at Mend, athletes and patients with a diagnosis of labral tears or FAI are able to return to sport following a treatment plan involving manual therapy, exercise, biome- chanics evaluation and modifications (ie gait analysis), and education.

When to seek Physical Therapy for Hip Pain and Injury
Athletes and patients with anterior hip and groin pain, loss of hip range of motion, and disability should be referred to Physical Therapy for conservative management.
Pain mainly in the groin (sensitivity .96-1.0) and a subjective report of hip/groin pain with clicking, locking, and giving way (sensitivity 1.0, specificity .85) may assist in the diagnosis of an acetabular labral tear(10,11).
References
1. Ganz R, Parvizi J, Beck M, et al. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res 2003(417):112–20.
2. Collins JA, Ward JP, Youm T. Is prophylactic surgery for femoroacetabular impingement indicated? A systematic review. Am J Sports Med 2014;42:3009–15.
3. Reiman, M. Femoracetabular Impingement Surgery: Are we moving too fast and too far beyond the evidence? Br J Sp Med. 2015. 0:1-6.
4. Montgomery SR, Ngo SS, Hobson T, et al. Trends and demographics in hip arthroscopy in the United States. Arthroscopy 2013;29:661–5.
5. Frank, J. et al. Prevalence of FAI imaging findings in asymptomatic volunteers. A systematic review. Arthroscopy. 2015:1-6.
6. Nardo, L. et al. FAI: Prevalent and Often Asymptomatic in Older Men: The Osteoporotic in Men Study. Clin Orthop Relat Res. 2015
7. Hunt D, Prather H, Harris Hayes M, et al. Clinical outcomes analysis of conservative and surgical treatment of patients with clinical indications of prearthritic, intra-articular hip disorders. Pm R 2012;4:479–87.
8. Ayeni OR, Farrokhyar F, Crouch S, et al. Pre-operative intra-articular hip injection as a predictor of short-term outcome following arthroscopic management of femoroacetabular impingement. Knee Surg Sports Traumatol Arthrosc 2014;22:801–5.
9. Kemp JL, Collins NJ, Makdissi M, et al. Hip arthroscopy for intra-articular pathology: a systematic review of outcomes with and without femoral osteoplasty. Br J Sports Med 2012;46:632–43.
10. Keeney JA, Peelle MW, Jackson J, et al. Magnetic resonance arthrography versusarthroscopy in the evaluation of articular hip pathology. Clin Orthop Relat Res 58 2004;429:163–9.
11. Burnett RS, Della Rocca GJ, Prather H, et al. Clinical presentation of patients with tears of the acetabular labrum. J Bone Joint Surg Am 2006;88:1448–57.







