
Ankle Sprain Injuries
Ankle sprains are one of the most common orthopedic injuries with an annual incidence of 7 sprains per 1000 individuals(1).
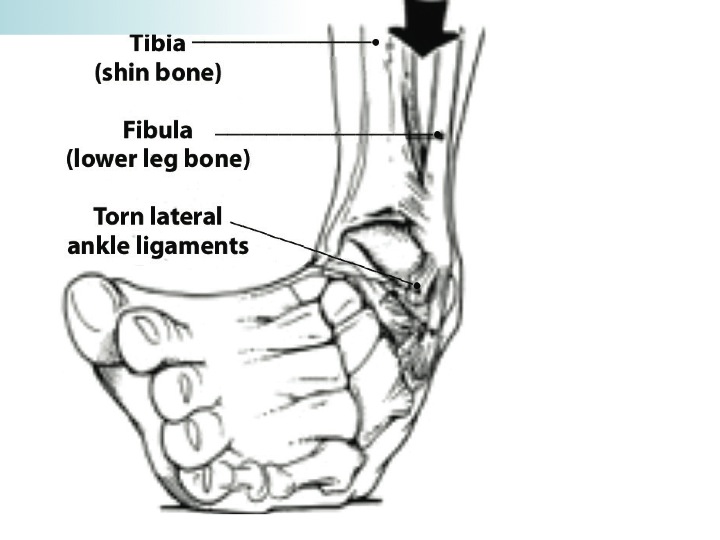
Lateral ankle sprains involving the outside of the ankle account for 85% of these sprains (see picture) and involve flexed and inverted foot(2).
Authors reports up to 72% of individuals who sustain an ankle sprain will report symptoms at 6 month follow up(4).
Grade I and II injuries, the least severe on a 3 point scale, are most likely to reoccur and may lead to chronic symptoms of instability(5).
Physical Therapy Interventions
Physical Therapy clinical practice guidelines promote the utilization of early protection and controlled motion following acute ankle sprains.
Patients with ankle sprain often demonstrate reduced hip motor performance which may increase their risk to future injuries. PT aims to correct these imbalances throughout the lower quarter to return clients to their prior levels of activity.
Authors recommend a multimodal treatment program consisting of early weight bearing, manual therapy, exercise and balance interventions to reduce pain and improve function(15).
Physical Therapy Evidence

Evidence supports the implementation of weight bearing, with or without assistive devices, following ankle sprains over non weight bearing(13).
Research has reported the utilization of R.I.C.E. (rest, ice, compression, and elevation) may be inferior to a Physical Therapy approach consisting of manual therapy and R.I.C.E interventions6.
A more effective treatment program designed to reduce pain, disability, and prevent recurrence of ankle injuries consists of manual therapy, balance/proprioceptive training, and return to sport exercise prescription(15).
Whitman et al. conducted a prospective study of 85 patients with acute ankle sprains and noted 75% of patients demonstrated an immediate improvement in symptoms and function in the first week of a manual therapy (see picture above) and exercise approach provided by Physical Therapists(8).
A recent systematic review demonstrated improved pain, improved motion, and decreased disability following manual therapy interventions in patients with ankle sprains(12).
Researchers reported restoring range of motion and decreasing pain processing from joints of the lower extremity may facilitate an earlier return to an exercise program.
Cleland et al. reported a formal Physical Therapy program consisting of manual therapy and exercise was more effective and efficient than a home program for patients with ankle sprain at both 4 weeks and 6 months after their sprain(10).
Balance training programs designed to reduce postural sway, improve joint stability and function, and prevent reoccurrence are prescribed following acute ankle sprains(14)

When to Schedule an Appointment
Patients should seek out Physical Therapy services following acute ankle injuries to be effectively screened for the aforementioned interventions. Appropriate candidates will be treated effectively with manual therapy, exercise and balance training, sport specific exercise interventions to facilitate return to sport and to prevent recurrence.
References
1. Almeida SA et al. Epidemiological patterns of musculoskeletal injuries and physical training. Med Sci Sp Ex. 1999;31:1176-1182
2. Ferran NA, Maffulli N. Epidemiology of sprains of the lateral ankle ligament complex. Foot Ankle Clin. 2006;11:659-662.
3. Bachmann, L. et al. Accuracy of Ottawa ankle rules to exclude fractures of the ankle and mid foot. A systematic review. BMJ. 2003;326:417
4. Braun, BL. Et al. Effects of ankle sprain in a general clinic population 6-18 months after medical evaluation. Arch Fam Med. 1999;8:143-149.
5. Malliaropoulos N, Ntessalen M, Papacostas E, Longo UG, Maffulli N. Reinjury after acute lateral ankle sprains in elite track and field athletes. Am J Sports Med. 2009;37:1755-1761.
6. Green T, Refshauge K, Crosbie J, Adams R. A randomized controlled trial of a passive accessory joint mobilization on acute ankle inversion sprains. Phys Ther. 2001;81:984-994
7. Eisenhart AW, Gaeta TJ, Yens DP. Osteopathic manipulative treatment in the emergency department for patients with acute ankle injuries. J Am Osteopath Assoc. 2003;103:417-421.
8. Whitman JM, Cleland JA, Mintken PE, et al. Predicting short-term response to thrust and nonthrust manipulation and exercise in patients post inversion ankle sprain. J Orthop Sports Phys Ther. 2009;39:188-200
9. Truyols-Dominguez, S. et al. Efficacy of Thrust and Nonthrust Manipulation and Exercise With or Without the Addition of Myofascial Therapy for the Management of Acute Inversion Ankle Sprain: A Randomized Clinical Trial. J Orthop Sports Phys Ther 2013;43(5):300-309.
10. Cleland et al. Manual physical therapy and exercise versus supervised exercise program in the management of patients status post inversion ankle sprain. A multi centered trial. JOSPT. 2013.
12. Loudon JK, Reiman MP, Sylvain J. The efficacy of manual joint mobilisation/ manipulation in treatment of lateral ankle sprains: a systematic review. Br J Sports Med 2014;48: 365–370.
13. Kerkhoffs GM, Rowe BH, Assendelft WJ, Kelly KD, Struijs PA, van Dijk CN. Immobilisation for acute ankle sprain. A systematic review. Arch Orthop Trauma Surg. 2001;121:462-471.
14. Webster KA, Gribble PA. Functional rehabilitation interventions for chronic ankle instability: a systematic review. J Sport Rehabil. 2010;19:98-114.
15. Martin, R. et al. Ankle Stability and Movement Coordination Impairments: Ankle Ligament Sprains. Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability and Health From the Orthopaedic Section of the American Physical Therapy AssociationJ Orthop Sports Phys Ther. 2013;43(9):A1-A40.