

The Centers for Disease Control, American College of Sports Medicine (ACSM) and American Heart Association recommend >5 days of week of moderate or >3 days per week vigorous cardiorespiratory (aerobic) exercise per week to improve fitness and reduce risk of illness and disease(1). Specifically, this dosage of exercise has been shown to reduce all cause mortality and reduce the risk of developing coronary heart disease, stroke, type 2 diabetes, and cancer(1). Also of note is the positive impact of exercise on our mental health including prevention or improvement of anxiety, depression, and other mild psychological disorders, as well as, improvement in quality of life and a lower risk of cogni- tive decline and and dementia(2). The majority of our athletes are reaching or exceeding this threshold of physical activity and receiving these positive benefits, but a percentage of these athletes may be at risk of illness or disease at higher levels of exercise.
Musculoskeletal injury is the most common risk associated with exercise, but a cardiovascular event including sudden death is the most serious. Prior research has demonstrated a risk of an acute myocardial infarction (heart attack) with vigorous aerobic exercise (jogging) particularly amongindividuals with underlying heart disease, often without signs and symptoms, or among those who initiate vigorous exercise from a sedentary lifestyle. In younger athletes, <30 in males and <40 in females, the underlying cause of cardio- vascular injury is likely congenital in nature (heart defect, arrythmias) and our ability to accurately screen these causes with a participation exam is debateable in the literature. Fortunately, these events in younger athletes are rare approximately 1 event in 133,000 and 769,000 men and women, respectively(3). The American Heart Association recommends cardiovascular screening for high school and college age individuals at 2 and 4 year intervals or more frequently for individuals with known disease.
As we age our risk for cardiovascular events (males>females) with exercise increases, regardless of other risk factors such as smoking and high blood pressure. Population data reports a yearly incidence of 1 acute cardiovascular event in between 500 to 3900 adults each year(4). This incidence increases substantially in individuals with known cardiovascular disease and prior history of events with exercise. In trained individuals meeting the cardiovas- cular standards reported above the relative risk of an acute cardiovascular event decreases substantially to approxi- mately 1/10th that of a sedentary individual(5). It is clear from the literature and guidelines individuals must determine their risk of injury and illness with aerobic exercise and adjust their exercise volume appropriately. In Table 1 below, risk factors for exercise are defined for a group of modifiable and non modifiable categories. In addition, a HDL level above 60 mg/dl is considered a negative risk factor and reduces risk for events with exercise.
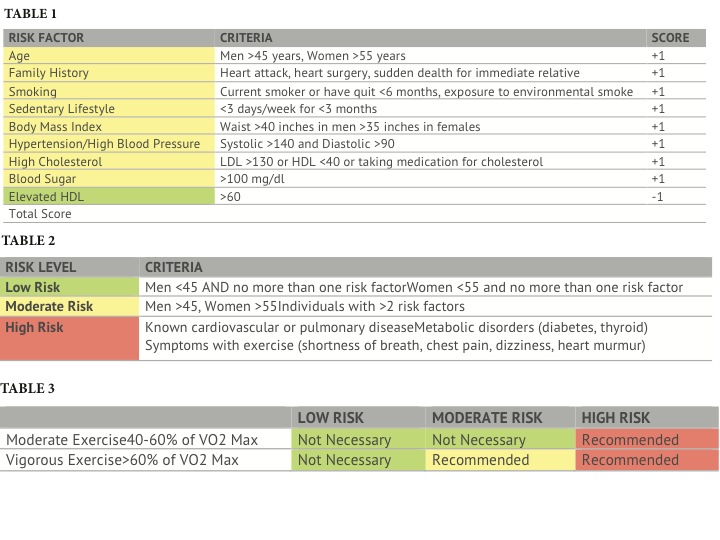
Each active individual should identify how many risk factors they have in order to gauge their risk for a cardiovascular event with exercise. For example, a 46 year old male with high blood pressure or taking high blood pressure medication has two risk factors. In Table 2 we can determine the American College of Sports Medicine Risk Level based on this total score. As you can see men over 45 and women over 55 are at moderate risk for injury irrespective of their health or risk factors. Our example above indicates this male is a moderate risk for a cardiovascular event with exercise.
In our final step, we need to determine how much of a physician examination or supervision is needed to perform either moderate or vigorous exercise. In our example, an individual at moderate risk should meetwiththeirphysician prior to performing vigorous exercise to reduce their risk of a cardiovascular event.
In closing, an appropriate exercise prescription may be one of the most powerful weapons to ward off disease, illness, and physical and cognitive decline with exercise. As we move to reach the thresholds associated with these benefits and our respective sports we must understand how to mitigate any risk associated with this training. Our athletes are encouraged to seek out their primary care physicians based on their risk factors and individual history prior to engaging in exercise. An excellent and quick screening chart is the Physical Activity Readiness Questionnaire (https://www.acsm.org/docs/current- comments/whentoseeadoctortemp.pdf ) which is another option to gauge your risk with exercise. Further information can be found at acsm.org or contact the experts at MEND PT.
References
1. American College of Sports Medicine. Position Stand. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults: Guidance for Prescribing Exercise. Medicine and Science in Sport and Exercise. 2011
2 Paterson DH, Warburton DE. Physical activity and functional limitations in older adults: a systematic review related to Canada’s Physical Activity Guidelines. Int J Behav Nutr Phys Act. 2010; 7:38.
3 VAN CAMP, S. P., C. M. BLOOR, F. O. MUELLER, R. C. CANTU, and H. G. OLSON. Nontraumatic sports death in high school and college athletes. Med. Sci. Sports Exerc. 27:641–647, 1995.
4 American College of Sports Medicine. Position Statement. Exercise and Acute Cardiovascular Events: Placing Risks into Perspective. Medicine and Science in Sport and Exercise. 2007
5 MITTLEMAN, M. A. Trigger of acute cardiac events: new insights. Am. J. Med. Sports 4:99–102, 2005.