
Pickleball continues to grow rapidly, but so do lower extremity injuries, particularly involving the Achilles tendon. The combination of quick acceleration, deceleration, and repetitive loading places significant strain on this structure. Research in sports medicine and tendon physiology consistently shows that Achilles injuries are rarely sudden events. Instead, they are typically the result of cumulative overload and missed early warning signs.
For coaches and players, the ability to identify risk early is critical. Below is a research-informed guide to understanding Achilles injury risk and a simple, clinically grounded self-screening process.
Why the Achilles Is at Risk in Pickleball
The Achilles tendon functions like a spring, storing and releasing elastic energy during movement. In sports involving repeated acceleration and deceleration, that spring is loaded frequently and at high force. Research in sports biomechanics shows the Achilles can experience forces up to 6–8 times body weight during running and jumping activities (Komi, 1990; Maffulli et al., 2004).
In pickleball, similar loading patterns occur during lunging for dinks, pushing off for lateral movement, and accelerating toward the kitchen line. Repeated loading without sufficient recovery or strength adaptation can lead to tendon irritation, commonly referred to as tendinopathy, and in more severe cases, partial or complete rupture (Magnusson and Kjaer, 2019).
Common Early Warning Signs
Achilles tendon injuries are typically preceded by a gradual onset of symptoms rather than a single event. Clinical research consistently identifies the following early indicators
- Morning stiffness in the back of the ankle
- Tenderness 1–2 inches above the heel bone
- Pain that decreases during activity but returns afterward
- Reduced push off power or perceived “sluggishness”
- Persistent calf tightness
Morning stiffness, in particular, is considered one of the most sensitive indicators of tendon overload and early tendinopathy (Silbernagel et al., 2007). Ignoring these symptoms increases the likelihood of progression to more serious injury.
Simple Self-Screen for Achilles Risk
This quick screening can be performed at home or courtside. While it is not diagnostic, it is supported by clinical principles used in sports physical therapy to identify early tendon dysfunction.
- Single-Leg Heel Raise Test
Stand on one leg and rise onto your toes in a controlled manner.
What to look for
- Ability to perform 15–20 repetitions with good control
- Symmetry between sides in height and endurance
Red flags
- Pain above 3 out of 10
- Noticeable weakness or early fatigue
- Compensatory movement such as leaning or using momentum
Reduced heel raise capacity has been strongly associated with Achilles tendinopathy and decreased tendon function (Silbernagel et al., 2007).
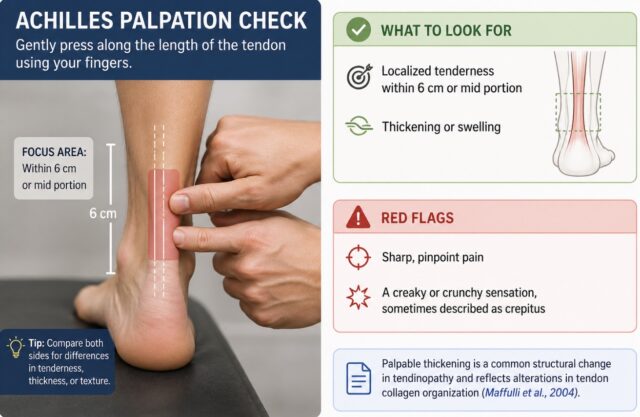
- Achilles Palpation Check
Gently press along the length of the tendon using your fingers.
What to look for
- Localized tenderness within 6 cm or mid portion
- Thickening or swelling
Red flags
- Sharp, pinpoint pain
- A creaky or crunchy sensation, sometimes described as crepitus
Palpable thickening is a common structural change in tendinopathy and reflects alterations in tendon collagen organization (Maffulli et al., 2004).
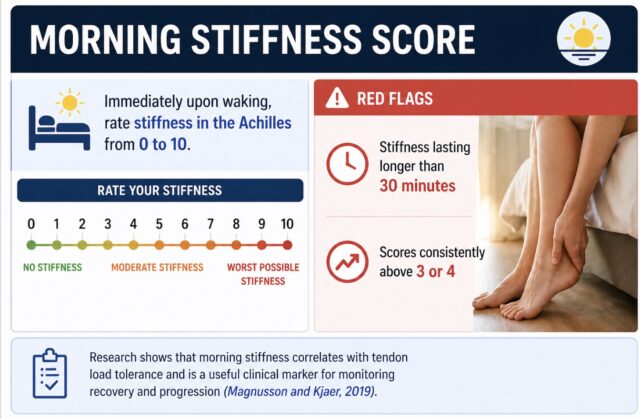
- Morning Stiffness Score
Immediately upon waking, rate stiffness in the Achilles from 0 to 10.
Red flags
- Stiffness lasting longer than 30 minutes
- Scores consistently above 3 or 4
Research shows that morning stiffness correlates with tendon load tolerance and is a useful clinical marker for monitoring recovery and progression (Magnusson and Kjaer, 2019).
- Hop Test
Stand on one leg and perform small, controlled hops.
What to look for
- Smooth, elastic movement
- Equal performance on both sides
Red flags
- Pain during hopping
- Hesitation or inability to generate spring
Plyometric tolerance reflects the tendon’s ability to store and release energy efficiently, which is often impaired early in tendinopathy (Komi, 1990).
- Calf Flexibility Check
Perform a standing calf stretch against a wall. Perform a half kneeling position and move your knee to the wall as far as possible without the heel lifting. Then measure the distance between your foot to wall.
What to look for
- Similar flexibility on both sides (ideal is 9 cm from toe to wall)
- A comfortable stretch without pain
Red flags
- Significant asymmetry
- Stretch reproduces Achilles pain
Limited calf flexibility can increase strain on the Achilles tendon during dynamic movements (Magnusson et al., 2008).
- Thompson Test (Rupture Screen)
This is a quick screening test commonly used in clinical settings to assess for a possible Achilles tendon rupture (Thompson, 1962).
How to perform
- Lie face down with your feet hanging off the edge of a bed or bench
- Have someone gently squeeze the calf muscle
What to look for
The foot should automatically point downward (plantarflex) when the calf is squeezed
Red flags
- Little or no movement of the foot
- A delayed or weak response compared to the other side
A positive Thompson test is highly sensitive for detecting a complete Achilles rupture and should be treated as a medical urgency requiring immediate evaluation.
How to Interpret Your Results
Low Risk
- No pain
- Symmetrical strength and mobility
- No morning stiffness
- Continue playing while maintaining strength and recovery habits
Moderate Risk
- Mild pain between 1-3 out of 10
- Slight asymmetry or stiffness
- Reduce intensity, incorporate calf strengthening, and monitor symptoms closely
High Risk
- Pain greater than 3 out of 10
- Weakness, swelling, or difficulty with hopping
- Pause high-impact activity and consult a physical therapist for evaluation
Take Action Before It Becomes an Injury
If you or your athletes are noticing early signs such as morning stiffness, reduced calf strength, or pain during play, this is the ideal time to intervene.
As a physical therapist specializing in movement and sports performance, I help pickleball players identify injury risk early, build tendon strength and resilience, and return to play safely and confidently.






