By: John Crawley, PT, DPT, OCS
How Pulley Injuries Occur: The Biomechanics
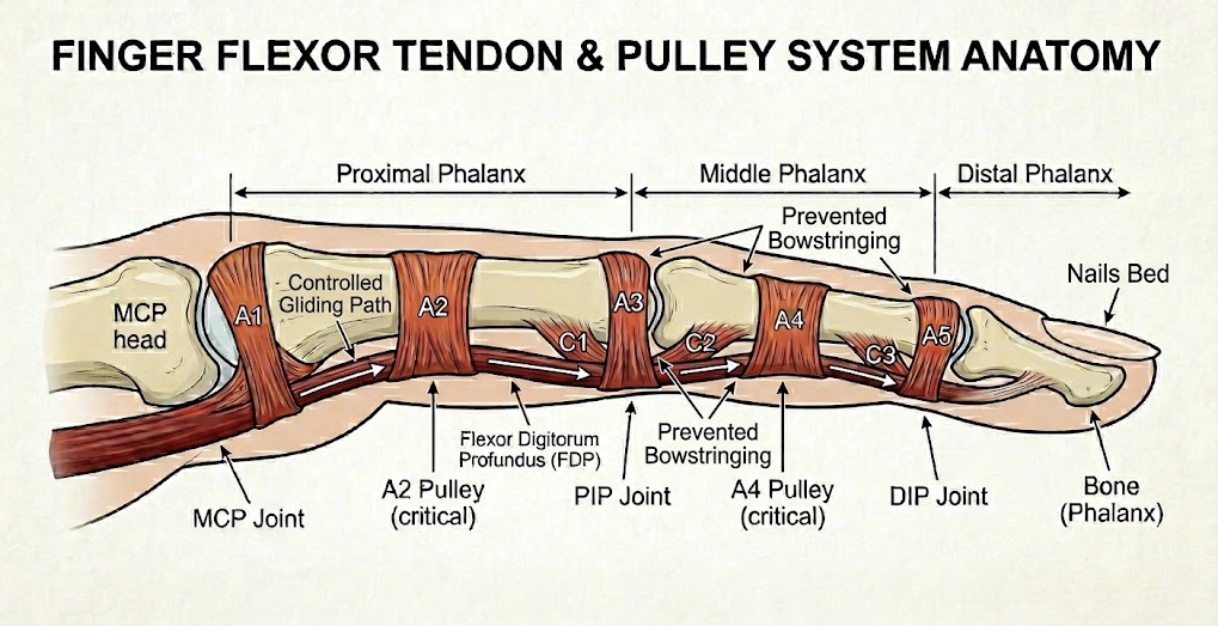
Your fingers don’t actually contain muscles; they are moved by long tendons (flexor digitorum superficialis and profundus) that originate in your forearm. These tendons run down your fingers through a sheath, held tight to the bone by ligamentous tunnels called pulleys. Think of your finger like a fishing rod and the tendon like the fishing line. The pulleys are the small guide rings on the rod that keep the line from bowstringing. Keeping the tendon close to the bone improves the movement quality of the fingers and improves force production through the fingers to grip.
The Breaking Point: Ultimate Tensile Strength
- A2 Pulley Tolerance: Controlled cadaveric studies have shown that a healthy, intact A2 pulley fails at a mean direct peak force of approximately 380 N to 400 N (Crowley, 2016; Iruretagoiena-Urbieta et al., 2020). However, this limit varies significantly depending on the age and conditioning of the individual, spanning from roughly 153 N in compromised tissue up to 569 N in robust, healthy male specimens (Larsson et al., 2022).
- A4 Pulley Tolerance: Because it is structurally thinner and possesses less cross-sectional area, the A4 pulley demonstrates lower mechanical tolerance, typically failing under significantly less force than the primary A2 structure.
Crimp Physics & Fingertip Multiplication
- The 3-to-4x Multiplier: Due to the severe mechanical disadvantage of the closed crimp grip, the internal force exerted outward against the A2 pulley is 3 to 4 times greater than the actual external force applied at the fingertip (Crowley, 2016).
- Crimp vs. Open Hand: Biomechanical modeling indicates that forces acting on the A2 pulley are up to 31.5 times higher when utilizing a strict crimp grip compared to an open-hand hanging grip on a sloper (Vigouroux et al., 2006).
- Real-World Loading: In real-world climbing, a recreational climber easily exposes the A2 pulley to standard working loads of around 380 N dynamically, whereas a sharp foot slip or sudden dynamic catch can cause instantaneous shock loading to spike up to 450 N or higher on a single finger, surpassing its ultimate tissue failure threshold (Crowley, 2016; Larsson et al., 2022).
The Climber’s Paradox: Why Do They Tear?
If a single A2 pulley can hold 90 pounds, you might wonder why they tear so easily when you have four other fingers and two feet sharing your body weight. The answer lies in the leverage and physics of the crimp grip.
When you place your finger into a sharp, closed crimp, the sharp bend of the joint creates a mechanical disadvantage. The force exerted outward against the pulley is significantly higher than the force your fingertip is actually applying to the climbing hold.
Real-World Force Spikes
In a controlled, static environment, your pulleys are remarkably resilient. However, climbing is rarely static. Pulleys typically fail due to two compounding factors:
1. Dynamic Shock Loading (The Foot Slip, deadpointing, catching a hold wrong)
If you are pulling hard on a hold and a foot blows, your body drops. The sudden, eccentric load can instantly double or triple the force on your fingers. The rapid force spike will exceed the pulley’s load tolerance and rupture.
2. Cumulative Fatigue (Repetitive Micro-Trauma)
Connective tissues like ligaments and pulleys exhibit hysteresis—meaning they lose a bit of their elastic tolerance when subjected to repetitive, heavy stress without enough rest. If you crimp a lot on hard project after project, the ultimate breaking strength of the tissue temporarily drops. A pulley that could normally withstand 400N may only be able to withstand 300N after repeated stress with inadequate rest time between attempts or sessions.
The Good News: Tissue Adaptation
The 400 N limit isn’t entirely fixed. Like bone and tendon, pulleys are living tissue that adapt to mechanical stress over time (Wolff’s Law).
Through years of progressive, safe loading (like consistent hangboarding and climbing), a seasoned climber’s pulleys will actually become thicker, stiffer, and capable of withstanding higher peak forces than those of a beginner. The key is giving them the months and years of gradual stimulus they need to build that armor.
Symptoms of a Pulley Injury
Pulley injuries range from Grade I (a minor strain/micro-tearing) to Grade IV (multiple ruptured pulleys with joint instability). Depending on the severity, you’ll notice a few classic signs:
- The Dreaded “Pop”: In moderate to severe tears (Grade II-IV), climbers often report hearing or feeling a distinct, audible pop or snap followed by immediate pain.
- Localized Pain and Swelling: The palmar side of the finger (usually right between the knuckles for an A2 injury) will be incredibly tender to the touch. Swelling and bruising often develop within 24 hours.
- Pain with Active Flexion: Crimping, pinching, or even just making a fist will hurt.
- Bowstringing: In severe cases where multiple pulleys are completely ruptured, you can actually see or feel the tendon lifting away from the bone when you try to flex your finger against resistance.
How a PT Examines a Hurt Finger
When you come into the clinic with a finger injury, the goal is to figure out exactly what structure is affected and how badly it’s injured. With that information a successful treatment plan can be made. Here is how a clinical exam typically goes down:
1. Subjective History
The exam begins with a conversation about your injury. During that conversation information will be gathered about your climbing history, how often you climb, how hard do you climb, what do you do for training, what kind of grips do you use, and have you had any other climbing injury. From there you will be asked exactly what position your hand was in, whether your foot slipped, if you heard a pop, and how quickly the swelling set in. The goal of this portion of the exam is to understand the environment, behaviors, and situation that contributed to the injury.
2. Palpation and Visual Inspection
As a part of the physical exam a PT will look for swelling, bruising, and any obvious structural changes. Palpation on (press on) specific zones of your finger can help hone in the clinician to where the injury was sustained and give information about what structures are involved.. Precise tenderness directly over the A2 pulley (base of the finger) or A4 pulley (middle phalanx) is a strong indicator of a pulley issue rather than a tendon tear or joint capsule sprain.
3. Range of Motion (ROM) & Flexibility Testing
Active and passive range of motion will be looked at. Range of motion restriction or where the pain is felt can help guide the clinician toward the problem tissue.
- Resisted Diagnostics (The “Climber Testing”)
This portion of the exam is one of the more important steps. Determining the load tolerance of the various grip and where pain is felt can indicate the severity of the injury and help to frame the rehabilitation program to resolve the finger pain.
- Isolated DIP/PIP Flexion: Here the fingers joints will be isolated and loaded. This gives information about the tendons, pulley’s, and joints.
- Climbing Specific Grip Load Testing: Testing here focuses on determining which grips are painful or pain free. Additionally, the amount of force produced relative to the unaffected side can suggest the extent to which the pulley or other finger tissue is injured.
- Diagnostic Imaging (Ultrasound)
Diagnostic ultrasound can be used to visualize the finger in real time. This allows the clinician to observe the function of the tendon under load. In some partial tears and in full ruptures bowstringing can be observed. If there is no bowstringing and low levels of pain with good force production, it is likely that there is a low grade sprain. If there is a lot of pain, low force production, and observable bowstringing than a high grade sprain is likely. It can also be used to help with differential diagnosis to rule out/in the presence of tenosynovitis.
If you’ve recently tweaked your finger in the Boulder, Denver, Longmont, or Lafayette area, the best immediate move is to decrease or stop climbing, avoid gripping a heavy object), and get it looked at by a professional. When correctly identified, effective rehab programs can be started. These plans take time to execute, but have excellent outcomes.
References
Crowley, T. (2016). The flexor tendon pulley system and rock climbing. Journal of Hand and Microsurgery, 4(1), 25–29. https://doi.org/10.1007/s12593-012-0061-3 Cited by: 79
Iruretagoiena-Urbieta, X., De la Fuente-Ortiz de Zarate, J., Blasi, M., Obradó-Carriedo, F., Ormazabal-Aristegi, A., & Rodríguez-López, E. S. (2020). Grip force measurement as a complement to high-resolution ultrasound in the diagnosis and follow-up of A2 and A4 finger pulley injuries. Diagnostics, 10(4), 206. https://doi.org/10.3390/diagnostics10040206 Cited by: 14
Larsson, R., Nordeman, L., & Blomdahl, C. (2022). To tape or not to tape: annular ligament (pulley) injuries in rock climbers—a systematic review. BMC Sports Science, Medicine and Rehabilitation, 14(1). https://doi.org/10.1186/s13102-022-00539-6 Cited by: 7
Vigouroux, L., Quaine, F., Labarre-Vila, A., & Moutet, F. (2006). Estimation of finger muscle tendon tensions and pulley forces during specific sport-climbing grip techniques. Journal of Biomechanics, 39(14), 2583–2592. https://doi.org/10.1016/j.jbiomech.2005.08.027 Cited by: 227